
Introducing “Neurotech between wellness and medicine”

Introducing “Between wellness and medicine”
This article introduces Between wellness and medicine, a series of articles examining the growing market of consumer neurotechnology devices caught between medical and wellness regulation. Subscribe to receive them via email (select “Neurotech”).
The rise in wellness neurotechnologies
The wellness market has become a multi-trillion-dollar industry[1], featuring all manners of gadgets and gizmos aimed at improving sleep, fitness, and mental health, that blur the line between self-care and healthcare. The promise is simple: take charge of your health and well-being through continuous self-monitoring of biometric data, and receive algorithmically personalised insights – often via chatbots – without the need to speak to a doctor.
Within this lucrative industry, the consumerisation of neurotechnologies for mental health and wellbeing has taken hold. Technologies once confined to clinical practice and regulation, such as electroencephalography (EEG), now appear in simplified form in consumer wearables that, through non-invasive brain recording or stimulation, claim to improve sleep, elevate mood, sharpen focus, enhance productivity or alleviate stress. At a time when nearly half of Europeans report recent struggles with mental health[2], this segment has become a top priority in the wellness sector[3]. In fact, wellness is now the largest consumer segment of neurotechnology, and the most heavily backed by venture capital in Europe and North America.
This commercial momentum has important regulatory implications.
The regulatory grey zone
Non-invasive neurotechnologies once limited to medical use can now be miniaturised and embedded into consumer gadgets including headbands, headphones, glasses, watches, and even earbuds.

Image: Neurable
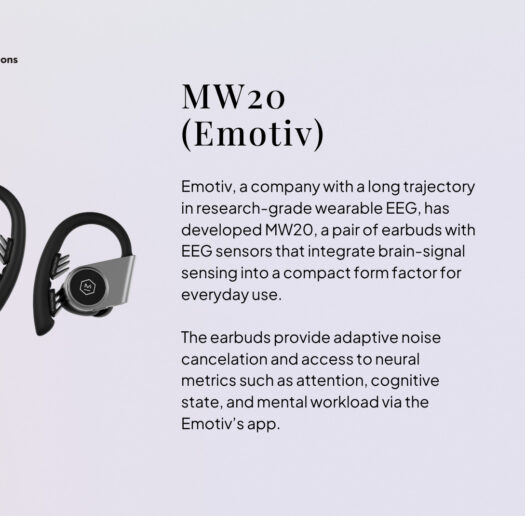
Image: Emotiv

Image: Interaxon
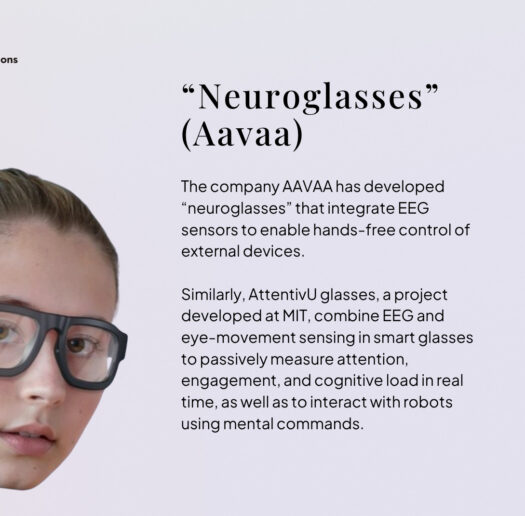
Image: Aavaa
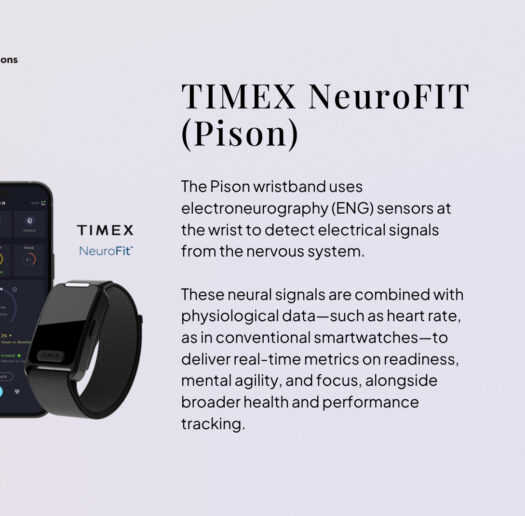
Image: Pison
Image: Meta
This consumerisation of former medtech complicates their classification as medical or consumer devices. As everyday wearables, they do not need to be classed as medical devices, but in practice neither are they purely recreational consumer technologies (unlike, for example, brain-computer interfaces for gaming) as their manufacturers often engage with health-adjacent narratives[4] and use cases[5].
Neurotechnologies are not unique in this regard. In fact, the Medical Device Coordination Group within the European Commission has issued manuals[6] to help member states handle those cases where it is not clear from the outset whether a given product is a medical device or not – so-called “borderline cases”. However, in practice, ambiguities remain. One reason is that, under the EU’s Medical Device Regulation (MDR) (and similarly under the FDA framework), what makes a non-invasive device “medical” is not the underlying technology, but its intended purpose[7] – namely, what the device is used for[8]. As a result, as engineering advances allow for the deployment of former non-invasive medical technologies through consumer form factors, the manufacturers’ claims about its intended purpose — and wording — make all the difference. For instance, a claim that a device “helps you relax” allows it to be sold as a consumer product, while a claim to “treat anxiety” is only allowed for products with medical certification — even if the underlying technology and its capabilities are identical.
Linguistic ambiguity is compounded by the fact that consumer products, unlike medical ones, are not required to demonstrate efficacy to enter the market. This creates a market “sweet spot” in which claims about intended purpose can be (legally) framed to sound as medical as possible – thereby conferring credibility – while remaining insufficiently medical to trigger formal medical scrutiny and, critically, the requirement to conduct clinical trials (see case 1 in the box below).
This could explain why most neurotechnology wearables are commercialised as consumer products[9]: a strategy that lowers regulatory and market entry barriers, but also increases the risk of health-adjacent claims that may mislead consumers[10] into interpreting these devices as medical products despite the absence of proven efficacy. At the same time, weak incentives to generate evidence in consumer markets risk foreclosing opportunities to leverage wearables and consumer-friendly form factors for meaningful health applications outside the clinic, such as mental health[11] support, preventative medicine[12],[13] or remote monitoring[14], despite the emerging evidence of their potential (see case 2). A further scenario is also technically possible: companies may underclaim the capabilities of a device to operate within consumer markets, where data protections are weaker, in order to begin building the body of evidence needed for a future medical use case (see case 3).
For companies the choice of which path to pursue commercialisation in is not trivial either, and it has profound implications for their strategies and long-term sustainability. In consumer markets, low-risk products can launch without evidence of efficacy, provided the products meet general safety[15] and data privacy standards (in the EU, the General Data Protection Regulation (GDPR)[16], AI Act[17], etc.), and do not make explicit medical claims. Hence, choosing the consumer route, unlike seeking medical certification under the EU’s MDR[18] or similar frameworks, avoids clinical trials and enables immediate access to a mass market and consumer data collection, an important asset in wellness markets. Paradoxically, and despite the lower barriers, the compliance route for consumer neurotechnologies in the EU is perhaps even more complex than for medical devices, as fragmented regulations leave gaps in consumer protection and add uncertainty for companies committed to responsible innovation (see case 4). The grey zone can also be grey for companies.
The regulatory grey zone in practice
The following examples, which are based on real cases, illustrate the ways in which current regulatory ambiguities condition market practices by creating different incentive structures. None of the examples below is legally wrong under existing regulation, but they illustrate the difficult position faced by consumers and companies in practice.
Case 1: Linguistic inflation / implied medicalisation. A company claims that using a device prevents burnout, which is associated with lower rates of depression and improved mental health, as studies cited on its website suggest. The company does not explicitly claim to treat depression (neither has generated evidence), but the medical-sounding language and website aesthetics may lead consumers to infer medical efficacy, despite the absence of explicit claims that would trigger medical device oversight.
Case 2: Evidence generation disincentives. A company seeks to certify a wearable product as a medical device, but insurance reimbursement in the EU is not guaranteed for low-risk wearable devices, and funding to conduct clinical trials is limited. An opportunity to contribute to healthcare is missed, not due to a lack of technical feasibility, but because of misaligned reimbursement incentives.
Case 3: Strategic underclaiming and data arbitrage. A company claims that a device helps with meditation, but in practice the EEG data collected during sessions can also be analysed for ADHD-related traits. The company therefore operates in consumer markets—where data protections are weaker—while incrementally building evidence for a potential medical use case, downplaying its capabilities in exchange for access to data.
Case 4: Chilling effects on responsible innovation. A group of researchers considers spinning out to develop a wellness device to improve sleep using a novel technology. However, the lack of regulatory cohesion around consumer neurotechnologies, combined with unresolved debates about how to protect brain data in consumer markets, discourages them from pursuing this effort.
How this series addresses regulatory ambiguity
In light of a growing health-adjacent market and the challenges this poses for consumers and innovators, the Centre for Future Generations has conducted an investigation to clarify the grey regulatory area from multiple perspectives. We have examined the market for wellness neurotechnologies, reviewed hundreds of company webpages and their products, analysed the language companies use to communicate products to consumers, explored the scientific evidence provided to substantiate their claims, and conducted a series of formal interviews and informal conversations with founders, innovators, academics and certification organisations to better understand their challenges. The findings inform the following pieces:
- Part 2 – Promise and peril: The piece tackles the growth of wellness neurotechnologies, companies’ positioning and marketing claims, and the risks that need to be overcome – particularly with respect to consumer protection – to realise the opportunities these technologies promise.
- Part 3 – How companies navigate the grey zone: This piece explores, through interviews with founders, the strategic decisions behind positioning their devices as consumer or medical, as well as the challenges they face under the current incentive structure and regulatory frameworks. It also highlights what founders say they need from regulators to enable responsible innovation to move forward .
- Part 4 – Clarifying the grey zone: EU governance of health-adjacent tech: This piece discusses the state of regulation for wellness neurotechnologies and, based on our compiled findings, proposes a novel governance framework to clarify the legal grey area.
Neurotechnology is not unique in facing such challenges, but it represents an early and particularly visible example of a broader class of health-adjacent consumer technologies that increasingly blur the established regulatory categories and, in doing so, risk undermining consumer protections and responsible innovation.
[1] Global Wellness Institute. (2024). The global wellness economy reaches a new peak of $6.3 trillion–and is forecast to hit $9 trillion by 2028. https://globalwellnessinstitute.org/press-room/press-releases/the-global-wellness-economy-reaches-a-new-peak-of-6-3-trillion-and-is-forecast-to-hit-9-trillion-by-2028/
[2] European Commission. (2023). Mental health – October 2023. Eurobarometer. https://europa.eu/eurobarometer/surveys/detail/3032
[3] McKinsey & Company. (2025). The Future of Wellness trends survey 2024. https://www.mckinsey.com/industries/consumer-packaged-goods/our-insights/future-of-wellness-trends
[4] Coates McCall, I., et al. (2019). Owning ethical innovation: Claims about commercial wearable brain technologies. Neuron, 102(4), 728–731. https://doi.org/10.1016/j.neuron.2019.03.026
[5] Wexler, A., & Thibault, R. T. (2018). Mind-reading or misleading? Assessing direct-to-consumer electroencephalography (EEG) devices marketed for wellness and their ethical and regulatory implications. Journal of Cognitive Enhancement. https://doi.org/10.1007/s41465-018-0091-2
[6]European Commission. (2025). Update: Manual on borderline and classification under Regulations (EU) 2017/745 and (EU) 2017/746 – September 2025. https://health.ec.europa.eu/latest-updates/update-manual-borderline-and-classification-under-regulations-eu-2017745-and-2017746-september-2025-2025-09-12_en
[7] European Medicines Agency. (n.d.). Medical devices. https://www.ema.europa.eu/en/human-regulatory-overview/medical-devices
[8] As long as the devices are low-risk. In Europe, implantable devices and non-invasive brain stimulation, whether consumer-oriented or medical, are legally classed as medical devices.
[9] Ienca, M., & Vayena, E. (2019). Direct-to-consumer neurotechnology: What is it and what is it for? AJOB Neuroscience, 10(4), 149–151. https://doi.org/10.1080/21507740.2019.1668493
[10] Wexler, A., & Thibault, R. T. (2018). Mind-reading or misleading? Assessing direct-to-consumer electroencephalography (EEG) devices marketed for wellness and their ethical and regulatory implications. Journal of Cognitive Enhancement. https://doi.org/10.1007/s41465-018-0091-2
[11] Borghare, P. T., et al. (2024). A comprehensive review on harnessing wearable technology for enhanced depression treatment. Cureus, 16(8), e66173. https://doi.org/10.7759/cureus.66173
[12] Menassa, M., et al. (2025).The future of healthy ageing: Wearables in public health, disease prevention and healthcare. Maturitas, Volume 196,108254,ISSN 0378-5122, https://doi.org/10.1016/j.maturitas.2025.108254
[13] Matias, I., et al. (2026). Digital biomarkers for brain health: Passive and continuous assessment from wearable sensors. npj Digital Medicine. https://doi.org/10.1038/s41746-026-02340-y
[14] Wall, C., et al. (2023). Beyond the clinic: The rise of wearables and smartphones in decentralising healthcare. npj Digital Medicine, 6, 219. https://doi.org/10.1038/s41746-023-00971-z
[15] European Union. (2023). General product safety regulation. https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=legissum:4670517
[16] European Union. (2016). Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). https://eur-lex.europa.eu/eli/reg/2016/679/oj
[17] European Union. (2024). Regulation (EU) 2024/1689 of the European Parliament and of the Council of 13 June 2024 laying down harmonised rules on artificial intelligence and amending Regulations (EC) No 300/2008, (EU) No 167/2013, (EU) No 168/2013, (EU) 2018/858, (EU) 2018/1139 and (EU) 2019/2144 and Directives 2014/90/EU, (EU) 2016/797 and (EU) 2020/1828 (Artificial Intelligence Act). https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32024R1689
[18] European Union. (2017). Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017 on medical devices, amending Directive 2001/83/EC, Regulation (EC) No 178/2002 and Regulation (EC) No 1223/2009 and repealing Council Directives 90/385/EEC and 93/42/EEC. https://eur-lex.europa.eu/eli/reg/2017/745/oj/eng
Authors

Laura Bernáez Timón
Fellow – Neurotechnology

Virginia Mahieu
Neurotechnology Director